Contact Info
-
45, Sector 7A Faridabad, 121006, IN
- thebonejointclinic@gmail.com
- +91 82872 71544
45, Sector 7A Faridabad, 121006, IN

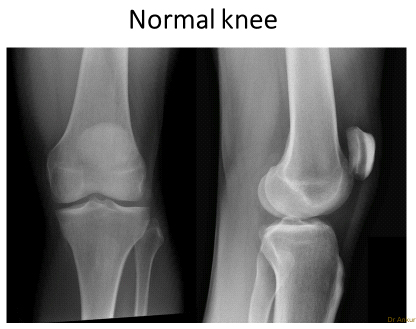
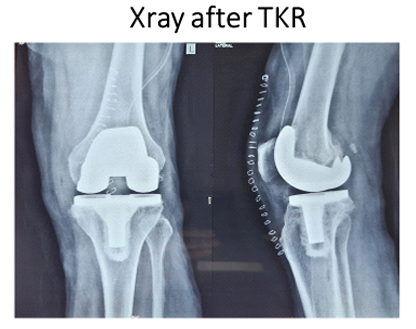
Total Knee Replacement' is a misleading term as your whole knee is not replaced! It only involves resurfacing the cartilage on the bones with new surfaces made of metal and polyethylene, which have been used successfully for many years

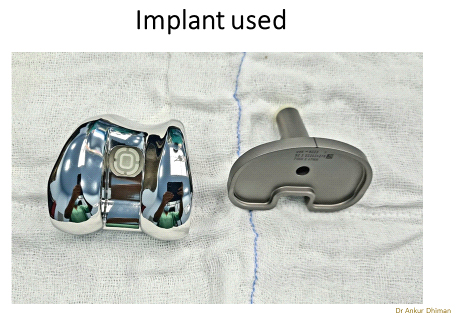
Yes, there are hundreds! We decide the most suitable one based on a thorough assessment of patient age, weight, activity level, bone quality, deformity, and ligaments. Do let us know if you have a preferred design in mind and are allergic to nickel, chromium or cobalt. We generally use usa imported Johnson & Johnson depuy knee.
Success depends on the surgeon and his team's experience, skills and technique in performing it, and the implant design. Now a day, due to high qualities of implant and advance surgery technique results are extra ordinary. Dr Ankur Dhiman use sub-vastus approach, he doesn’t cut the muscle to explore the joint and power of muscle remain healthy after operation. hence post-operatively recovery is very good.
No! We have performed knee surgery in persons upto the age of 90 years provided they have undergone detailed examination, investigations, and assessment by our physicians.
Our advanced surgical technique, even if they were severely bowed or knock-kneed than we can straightened it. We have developed special techniques to correct extremely deformed knees.
We have successfully operated on patients even if they are overweight (upto 145 kg!), diabetic, and have heart problems - provided they have undergone a complete examination, investigations, and assessment by our physicians. Diabetes and high blood pressure need to be controlled before surgery. Usually after bypass surgery or stenting, we follow the cardiologist's recommendation and delay surgery for 6 months.
If there is also a spinal problem (slipped disc, sciatica, spondylosis, canal stenosis), this will need careful examination and investigations (like MRI scan, EMG). Knee surgery will get rid of knee pain but not cure spine-related pain, numbness, and tingling in the legs, which will require assessment by a neurologist/spinal surgeon. If spinal and knee pain are equally severe, we can help you decide which surgery should be done first. TKR can be done after spinal surgery.
Most patients can stand and take a few steps the same evening after surgery, and next day will be able to use a chair and commode, walk with a stick/walker, and climb a few steps. If there's an elevator, you can start going out of your house at 2 weeks. After a month, you can climb stairs, drive, swim, take long walks, and travel.
Yes, post-operative physiotherapy is key point for recovery. To make your knee fully functional, good quality of physiotherapy is very helpful till 4-6 weeks
Most persons can drive 1 month after surgery.
Climbing stairs and sitting cross-legged on the floor. These are to be avoided, especially if you are overweight, to prevent excess load on your new knee and ensure that it lasts long.
Yes, you will be able to pick things up from the ground and reach low cupboards and drawers.
Walking, stationery cycling, swimming, yoga (preferably on a bed or sofa), doubles tennis and badminton, dancing, supervised weight training, and using a cross-trainer.
You will be shown how to climb a few steps the day after your surgery. We advise you to avoid climbing floors for 1month. Initially you may go up and down one foot at a time. Soon you will do stairs normally when your muscle strength and balance return.
Returning to normal varies from person to person depending on their condition before surgery usually taking 4-6 weeks and upto 6 months. Some stiffness, soreness and aching may last for 9-12 months.


